تستعرض هذه الدراسة أبحاث العلماء حول تأثيرات الصيام على الوقاية من السرطان وعلاجه، حيث تقدم رؤية شاملة من خلال تجميع المعلومات من دراسات أخرى. تشير النتائج إلى أن الصيام المتقطع قد يساعد في كبح نمو الأورام عن طريق تغيير الاستقلاب الخلوي، وتحسين الاستجابة المناعية، وتقليل الآثار الجانبية للعلاجات التقليدية مثل العلاج الكيميائي. على الرغم من أن الأدلة الأولية - خاصة عند الجمع مع العلاجات الجهازية - واعدة، إلا أن التنوع الاستقلابي للأورام والحاجة إلى مزيد من الدراسات السريرية تُظهر ضرورة الحذر عند تعميم النتائج. يؤكد هذا البحث أيضًا على أهمية تصميم تجارب معشاة ذات شواهد لتقييم فعالية الصيام الإسلامي كتدخل مساعد في السرطان. قد يفتح دمج العلاج الطبي الحديث مع أنظمة الصيام آفاقًا جديدة في إدارة السرطان، بشرط أن تحقق الأبحاث المستقبلية تقدمًا أكبر في وضع بروتوكولات آمنة للتطبيق.
الملخص
تعد الأنظمة الغذائية القائمة على الصيام نهجًا شائعًا يستخدمه الآلاف للمساعدة في التحكم بالوزن، وإراحة الأمعاء، وتحقيق فوائد صحية أخرى. في السنوات الأخيرة، أظهرت الأبحاث أن الصيام يمكن أن يقلل بعض عوامل الخطر وحتى يحسن أعراض أمراض خطيرة مثل السرطان. تبحث هذه الدراسة المراقبة في أحدث الدراسات المنشورة في المجلات الطبية حول الصيام وتأثيره على منع أو الوقاية أو علاج السرطان. الهدف من هذه الدراسة هو تقييم إمكانية تكييف ممارسة الصيام كفريضة دينية في الإسلام مع أحدث التطورات الطبية في مجال الصيام. تظهر نتائج هذه الدراسة أنه على الرغم من وجود أدلة على تأثير الصيام الإيجابي عند دمجه مع بعض علاجات السرطان الجهازية، إلا أن هناك حاجة إلى مزيد من التجارب السريرية للحصول على نتيجة واضحة وشاملة.
1. المقدمة
يُعتبر الصيام أحد أهم العبادات الدينية وفرضًا إلهيًا على المسلمين في شهر رمضان المبارك، كما ورد في الآيتين 183 و 184 من سورة البقرة. يؤكد هذا الأمر على التقرب إلى الله تعالى وتزكية الجسد والروح. الصيام الإسلامي، من الناحية الغذائية، يعني الامتناع عن الأكل والشرب خلال ساعات محددة من اليوم (من أذان الفجر إلى أذان المغرب). يأمر القرآن المسلمين بالصيام في الآية 183 من سورة البقرة، ويشجع عليه حتى للمرضى أو غير القادرين في الآية 184، مستخدمًا عبارة “وَأَن تَصُومُوا خَيْرٌ لَّكُمْ إِن كُنتُمْ تَعْلَمُونَ“. قام العديد من الباحثين بدراسة تأثيرات الصيام على الصحة الجسدية، وشيخوخة الخلايا، والعمر الطويل، والأمراض العصبية، والمناعة الذاتية، وأمراض القلب والأوعية الدموية، والأمراض الاستقلابية، وأثبتوا فوائده [1]. من بين هذه الدراسات، حصل العالم الياباني يوشينوري أوسومي على جائزة نوبل في الطب عام 2016 لإثباته أن الصيام ينشط عملية الالتهام الذاتي (عملية إعادة تدوير الخلايا وتجديدها) ويبطئ الشيخوخة [2].
ومع ذلك، فإن النقطة الحرجة في هذا البحث هي تأثير الصيام على الأفراد المرضى، حيث لم تظهر الدراسات الحالية آثاره الإيجابية أو السلبية بشكل قاطع. يُعتبر السرطان من أصعب أمراض العصر الحديث، وعادةً ما يُنصح المرضى باتباع نظام غذائي كامل ومتنوع. لكن الوضع يصبح أكثر تعقيدًا للمرضى المسلمين في رمضان، حيث تثير التوصيات حول الصيام أو عدمه مخاوف دائمة. غالبًا ما ينصح الأطباء بعدم الصيام أثناء العلاج وحتى لمدة عامين بعده. ومع ذلك، فإن الآثار المحتملة – الإيجابية أو السلبية – عالميًا تتطلب مزيدًا من البحث. بينما تركز بعض الدراسات على أضرار الصيام على الخلايا السرطانية وانتشارها، تشير دراسات رائدة أخرى إلى سلامته وحتى فوائده لمرضى السرطان.
وبالتالي، يبرز السؤال: أي النتائج أكثر موثوقية؟ وفي أي ظروف يمكن استخدام الصيام كعامل وقائي أو علاجي للسرطان؟ تبحث هذه المقالة المراقبة في الدراسات الحالية لتحديد الظروف التي قد يكون فيها الصيام مفيدًا للوقاية من السرطان أو علاجه.
2. خلفية البحث
يُعد الصيام أو الصيام المتقطع، سواء لعدة أيام في الأسبوع أو لساعات محددة يوميًا، نهجًا شائعًا يستخدمه الآلاف للمساعدة في التحكم بالوزن وإراحة الأمعاء وتحقيق فوائد صحية أخرى [3]. ظهرت أنظمة غذائية مختلفة تحاكي أنماط الصيام، مثل FMD وSTF وPFCR وIF، مصنفة حسب المدة والتغييرات الغذائية. بينما تشير بعض الدراسات إلى أن الصيام قد يحفز الخلايا السرطانية ويعزز الانتشار [4]، وأن تجويع الورم غير فعال بسبب اعتماد جميع الخلايا (سواء كانت سرطانية أم غير سرطانية) على الجلوكوز للتنفس [5]، فإن دراسات أخرى تبلغ عن نتائج مذهلة حول سلامة الصيام وحتى فوائده لمرضى السرطان. ومع ذلك، تم تسليط الضوء على هذه النتائج بحذر شديد [6].
تشير بعض الأبحاث إلى أن الصيام يمكن أن يكون، في حالات معينة، وسيلة للوقاية من أنواع معينة من الأورام الصلبة وعلاجها [7]. عند دمجه مع علاجات السرطان، قد تحد القيود الغذائية من تكيف الخلايا السرطانية وبقائها ونموها، مما قد يلعب دورًا رئيسيًا في هجوع السرطان [8-11]. قد يعزز أيضًا علاجات مثل العلاج الكيميائي والمناعي والهرموني [12-13] ويقلل من الآثار الجانبية للعلاجات الإشعاعية [14-15].
يبدو أن هذه الآثار الإيجابية مرتبطة بعوامل مثل انخفاض إنتاج الجلوكوز في الدم، وتحفيز الخلايا الجذعية لتجديد الجهاز المناعي، والتوازن الغذائي [11]. بالإضافة إلى ذلك، يؤثر الصيام بشكل كبير على استقلاب الدهون، ونشاط بكتيريا الأمعاء، وتناول السعرات الحرارية [16]، ويعزز إفراز الكوليسترول من الخلايا السرطانية [17]. وبالتالي، فإن الجمع بين الصيام والعلاج الكيميائي يبطئ تطور سرطانات مثل الثدي والجلد [18-19] ويزيد من إنتاج الخلايا اللمفاوية الأولية (CLPs) والخلايا اللمفاوية المتسللة للورم، مما يساعد في القضاء على الورم.
لذلك، لا يقلل تقييد السعرات الحرارية في الأنظمة الغذائية القائمة على الصيام من سمية علاجات السرطان في الخلايا السليمة فحسب [12-13]، بل يلحق أيضًا أضرارًا كبيرة بالخلايا السرطانية [6، 10]. بشكل عام، تُظهر مراجعة الأدبيات العلمية أنه على الرغم من أن التلاعب الغذائي بالعديد من المستقلبات يُظهر مزايا قبل سريرية واضحة ويظهر بعضها نتائج واعدة في التجارب السريرية، لا توجد إرشادات واضحة أو تعديلات غذائية موصى بها لمرضى السرطان. للوقاية من أنواع السرطان المختلفة أو علاجها، هناك حاجة إلى توصيات أو تركيبات غذائية مناسبة، حيث قد تختلف آثار هذه الأنظمة الغذائية اعتمادًا على النشاط الاستقلابي ومصادر الطاقة والاعتماديات الغذائية لكل نوع من أنواع السرطان [14].
3. منهجية البحث
3-1. منهجية البحث الديني والقرآني:
تعتمد هذه الدراسة على الآيتين 183 و 184 من سورة البقرة، مع الرجوع إلى التفاسير المعتمدة للقرآن الكريم. تم فحص الصيام كمفهوم رئيسي، ومقارنة الدراسات المستخلصة مع الأحكام الإسلامية حول الموضوع.
3-2. منهجية البحث العلمي:
تعتمد هذه الدراسة على مصادر علمية موثوقة، منشورة في قواعد بيانات مثل PubMed (MEDLINE) وScopus وEmbase، بالإضافة إلى مجلات Nature (2014-2024). شملت الكلمات الرئيسية: الصيام، FMD، STF، PFRC، DR، IF، السرطان، إلخ. تمت أولوية الدراسات ذات الاستشهادات العالية والتأثير الكبير.
4. تنفيذ البحث والنتائج والمناقشة
4-1. نقاط الضعف الاستقلابية للسرطان
تُظهر مسارات استقلاب المغذيات في الخلايا السرطانية كيف تعدل هذه الخلايا استقلابها لتلبية احتياجات الطاقة والهيكل [21]. تشمل هذه التغييرات زيادة امتصاص المغذيات وتفعيل المسارات البنائية داخل الخلايا. المصادر الغذائية الأساسية الثلاثة للخلايا السرطانية هي الجلوكوز والأحماض الأمينية والدهون.
- استقلاب الجلوكوز: يعمل الجلوكوز كمصدر رئيسي للطاقة، ويتم الحصول عليه من الغذاء أو تصنيعه في الكبد. يتم استقلابه عبر:
- تحلل السكر (Glycolysis): يتحلل الجلوكوز إلى بيروفات في السيتوبلازم، منتجًا ATP وNADH. تفضل الخلايا السرطانية تحلل السكر حتى في وجود الأكسجين (تأثير واربورغ) [22].
- التفسفر المؤكسد (Oxidative Phosphorylation): يدخل البيروفات الميتوكوندريا، مولّدًا المزيد من ATP عبر دورة حمض الستريك وسلسلة نقل الإلكترون. هذا المسار أكثر كفاءة ولكنه يعتمد على الأكسجين [23].
- دور اللاكتات: لم يعد يُعتبر اللاكتات مجرد نفايات، بل أصبح مصدرًا مهمًا للطاقة للعديد من الأورام، حيث قد يتجاوز استخدامه الجلوكوز في دورة حمض الستريك [24].
- استقلاب الفركتوز: يعمل الفركتوز أيضًا كمصدر للطاقة، حيث يتحلل عبر مسارات تحلل السكر. يمكنه إعادة برمجة المسارات الاستقلابية للبناء الحيوي وبقاء الخلية.
- استقلاب الأحماض الأمينية:
- الغلوتامين: حمض أميني غير أساسي يُحصل عليه من الغذاء أو تحلل العضلات أو المسارات داخل الخلايا. يتحول إلى α-ketoglutarate، مما يوفر وسطاء لدورة حمض الستريك ويساعد في تخليق الأحماض الدهنية [25].
- الأحماض الأمينية متفرعة السلسلة (BCAAs): تُستخدم الليوسين والأيزوليوسين والفالين لتخليق البروتين أو الطاقة.
- استقلاب الأحماض الدهنية: تعمل الدهون كمصدر كثيف للطاقة، وتأتي من الغذاء أو مخازن الجسم. أثناء نقص الغذاء، تتفكك الدهون إلى أحماض دهنية وجليسرول. تُؤكسد الأحماض الدهنية لإنتاج ATP، أو تساهم في تخليق الفوسفوليبيدات/الكوليسترول، أو تُخزن في الخلايا. في الكبد، تتحول الأحماض الدهنية إلى كيتونات، والتي قد تستخدمها بعض الأورام [26].
- تأثير نقص الأكسجين (Hypoxia): في حالات نقص الأكسجين، تزيد الخلايا السرطانية من تحلل السكر وتقلل إنتاج NADH لتلبية احتياجات الطاقة. لوحظت هذه المرونة الاستقلابية أيضًا في بعض الخلايا المناعية [22].
- نقاط الضعف الاستقلابية: تعتمد الخلايا السرطانية على مسارات استقلابية معينة للبقاء، والتي يمكن استهدافها علاجيًا – مثل تقييد الجلوكوز أو الغلوتامين أو استهداف مسارات مثل مسار البنتوز فوسفات. يعد فهم هذه المسارات أمرًا بالغ الأهمية لتصميم علاجات فعالة للسرطان.
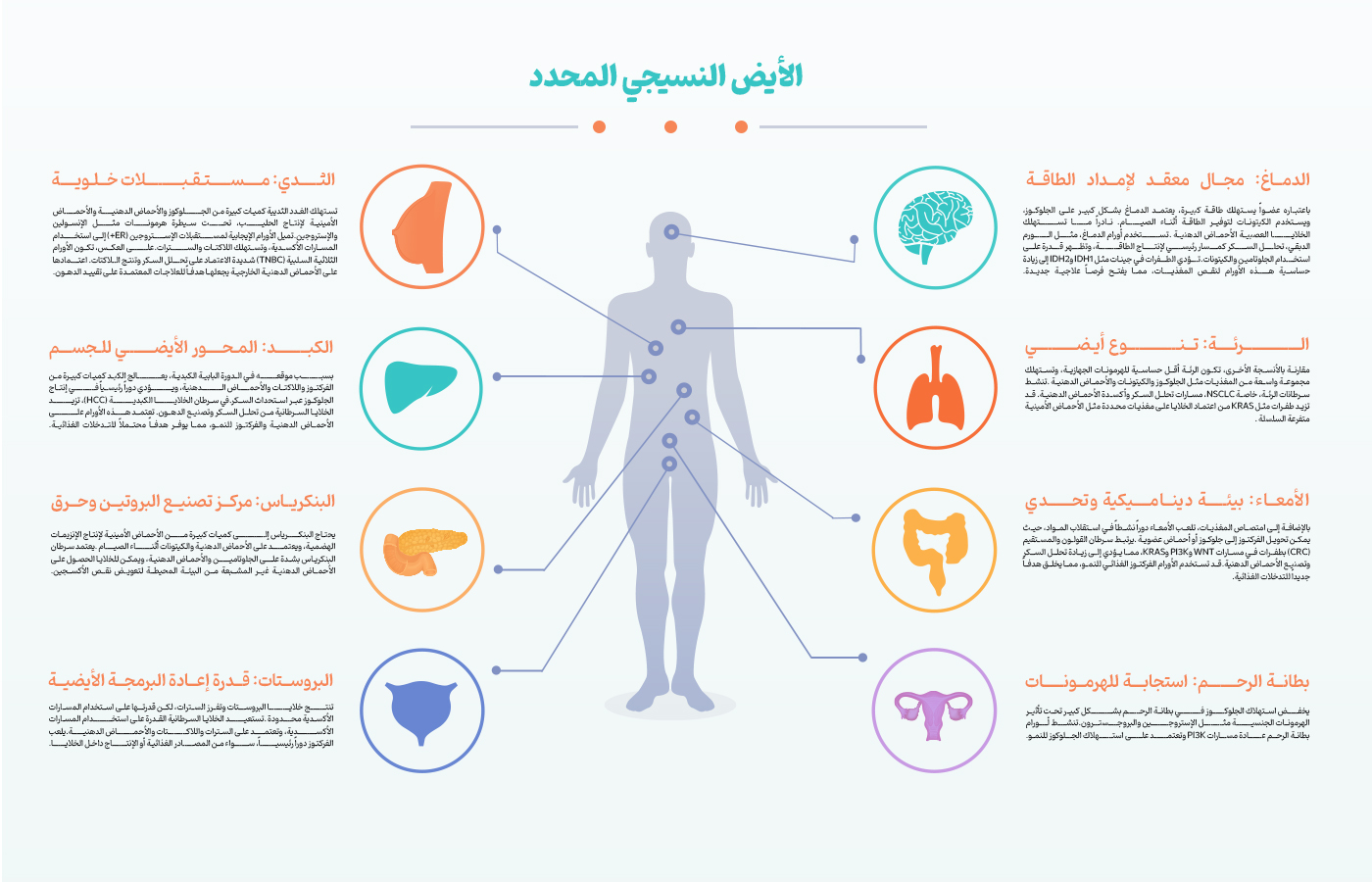
4-2. الاستقلاب النسيجي المحدد
تُظهر الأورام تغيرات استقلابية مميزة بناءً على أصلها النسيجي، مما يعكس التكيف مع بيئات مختلفة [27]. أمثلة رئيسية:
- الدماغ:
- الاستقلاب الطبيعي: يعتمد الدماغ بشدة على الجلوكوز، وأثناء الصيام، على الكيتونات. نادرًا ما تستخدم الخلايا العصبية الأحماض الدهنية [28-32].
- تغيرات السرطان: تستخدم أورام الدماغ (مثل الورم الدبقي) تحلل السكر كمسار رئيسي لإنتاج الطاقة، ولكنها قد تستخدم أيضًا الغلوتامين والكيتونات. تزيد الطفرات في جينات مثل IDH1 وIDH2 من اعتماد الورم على المغذيات، مما يوفر فرصًا علاجية جديدة.
- الثدي:
- الاستقلاب الطبيعي: تستهلك الغدد الثديية كميات كبيرة من الجلوكوز والأحماض الدهنية والأحماض الأمينية لإنتاج الحليب، بتنظيم من الإنسولين والإستروجين [33-38].
- تغيرات السرطان:
- تعتمد الأورام الإيجابية لمستقبلات الإستروجين (ER+) على المسارات المؤكسدة (تستهلك اللاكتات والسترات).
- الأورام الثلاثية السلبية (Triple-Negative) تعتمد بشدة على تحلل السكر وتنتج اللاكتات. قد يكون اعتمادها على الأحماض الدهنية الخارجية هدفًا للأنظمة الغذائية منخفضة الدهون.
- الكبد:
- الاستقلاب الطبيعي: يعالج الكبد كميات كبيرة من الفركتوز واللاكتات والأحماض الدهنية عبر الوريد البابي، ويُنتج الجلوكوز عبر استحداث السكر [39-45].
- تغيرات السرطان: يزيد سرطان الخلايا الكبدية (HCC) من تحلل السكر وتخليق الدهون، معتمدًا على الأحماض الدهنية والفركتوز – مما يوفر أهدافًا محتملة للتدخلات الغذائية.
- القولون:
- الاستقلاب الطبيعي: يلعب القولون دورًا نشطًا في امتصاص المغذيات واستقلابها (مثل تحويل الفركتوز إلى جلوكوز أو أحماض عضوية) [46-53].
- تغيرات السرطان: تزيد سرطانات القولون والمستقيم (CRC) مع طفرات WNT/PI3K/KRAS من تحلل السكر وتخليق الأحماض الدهنية. قد تستخدم الأورام الفركتوز الغذائي للنمو.
- البروستات:
- الاستقلاب الطبيعي: تنتج خلايا البروستات وتفرز السترات، ولكن لديها قدرة محدودة على استخدام المسارات المؤكسدة [54-56].
- تغيرات السرطان: تستعيد الخلايا السرطانية قدرتها على استخدام المسارات المؤكسدة، معتمدة على السترات واللاكتات والأحماض الدهنية. يلعب الفركتوز دورًا رئيسيًا، سواء من الغذاء أو التصنيع داخل الخلايا.
- الرئة:
- الاستقلاب الطبيعي: تستهلك الرئة الجلوكوز والكيتونات والأحماض الدهنية، مع حساسية أقل للهرمونات الجهازية [57-61].
- تغيرات السرطان: تنشط سرطانات الرئة (خاصة NSCLC) تحلل السكر وأكسدة الأحماض الدهنية. قد تزيد الطفرات مثل KRAS من اعتماد الخلايا على مغذيات معينة مثل BCAAs.
- البنكرياس:
- الاستقلاب الطبيعي: يحتاج البنكرياس إلى كميات كبيرة من الأحماض الأمينية لإنتاج الإنزيمات الهضمية، ويستخدم الأحماض الدهنية والكيتونات أثناء الصيام [62-65].
- تغيرات السرطان: تعتمد سرطانات البنكرياس بشدة على الغلوتامين والأحماض الدهنية، وقد تجمع الأحماض الدهنية غير المشبعة من البيئة لتعويض نقص الأكسجين.
- بطانة الرحم:
- الاستقلاب الطبيعي: يخضع امتصاص الجلوكوز في بطانة الرحم لتأثير هرمونات مثل الإستروجين والبروجسترون [66-69].
- تغيرات السرطان: تنشط أورام بطانة الرحم عادةً مسارات PI3K، معتمدة على استهلاك الجلوكوز للنمو.
الرؤية العلاجية: تقدم السمات الاستقلابية النسيجية فرصًا لتدخلات غذائية مستهدفة (مثل تقييد الجلوكوز أو أحماض أمينية أو دهون معينة) مع الأدوية، مما يفتح آفاقًا جديدة في علاج السرطان.
4-3. تصنيف الدراسات حسب نوع النظام الغذائي
قد تحسن التدخلات الغذائية علاج السرطان عن طريق:
- استنفاد المغذيات التي تغذي الأورام.
- تعزيز العلاج الإشعاعي/الكيميائي عبر تجويع الأورام.
- تعديل عوامل النمو أو المناعة الجهازية [3].
تشمل الأساليب:
- تقييد السعرات الحرارية (CR): خفض السعرات اليومية بنسبة 15-30% مع الحفاظ على توازن المغذيات الكبرى. يقلل CR من وزن الجسم وكتلة الدهون والأنسولين والهرمونات الدرقية ومعدل الاستقلاب [71-73]. منذ القرن العشرين، أظهر CR تأثيرات مضادة للأورام في الفئران، مما يقلل من الإصابة/التقدم/النقائل [74-77]. البيانات البشرية محدودة [78-80]. تجربة BWEL (المرحلة الثالثة) تقيّم CR في سرطان الثدي المبكر [83].
- أنظمة محاكاة الصيام (FMD):
- قد تأتي فوائد CR من فترات الصيام، وليس فقط تقييد السعرات [84-85].
- أظهرت تجارب سريرية صغيرة أن الصيام يقلل الهرمونات المحفزة للورم والآثار الجانبية، ويحسن جودة الحياة [86-87]. كما يغير الخلايا المناعية، مما قد يعزز الاستجابة المضادة للورم [88].
- التحديات: يصعب الحفاظ على الصيام طويل الأمد [89]. تحاكي أنظمة FMD (مثل نظام نباتي لمدة 5 أيام، 300-600 سعرة/يوم) فوائد الصيام [91].
- في الفئران، عززت دورات FMD فعالية العلاج [93-95]. التجارب البشرية جارية . [123-96]
- أنظمة منخفضة الكربوهيدرات جدًا (VLCD):
- أظهرت تجربة VLCD لمدة 12 أسبوعًا في سرطان المبيض/الرحم فقدانًا انتقائيًا للدهون، مع الحفاظ على الكتلة غير الدهنية وعدم تغير الدهون في الدم . [126-124]
- في سرطان الثدي، قلل VLCD حجم الورم أثناء العلاج الكيميائي، لكن النتائج تحتاج تفسيرًا حذرًا . [124]
- أنظمة منخفضة الدهون (LFD):
- تركز LFDs (<30% دهون) على الخضار والفواكه والحبوب الكاملة. تقلل بأمان من الوزن والكوليسترول وتناول الطعام [127-130].
- في سرطان الثدي، حسنت LFDs البقاء بعد التشخيص في مجموعات فرعية (تجارب WHI، WINS، WHEL) . [131-136]
- في سرطان البروستات، فوائد LFDs أقل وضوحًا، ربما بسبب تكيف الورم الاستقلابي [137].
- تدخلات أخرى:
- قد يؤدي تقييد أحماض أمينية محددة (مثل السيرين، الجلايسين، السيستئين، الميثيونين) إلى نتائج واعدة قبل السريرية، لكنها تفتقر إلى بيانات سريرية.
4-4. التدخلات الغذائية كمساعد للعلاج الإشعاعي
قد يعزز الصيام العلاج الإشعاعي عن طريق إضعاف إصلاح الحمض النووي للورم. أمثلة:
- يزيد تقييد الميثيونين من حساسية الأورام للإشعاع في الفئران [138].
- حسنت الأنظمة منخفضة الكربوهيدرات/الحالة الكيتونية البقاء في الورم الدبقي المتكرر (تجربةERGO2 ) للمرضى الذين حققوا مستويات منخفضة من الجلوكوز [141].
5. الخاتمة وتوجهات الأبحاث المستقبلية
يرى عامة الناس أن التغذية مهمة جدًا، خاصة للمرضى. ومع ذلك، في الطب الحديث الذي يعتمد على الأدوية والإشعاع، غالبًا ما يُنظر إلى النظام الغذائي على أنه داعم فقط. يعيد البحث الحديث استكشاف نقاط الضعف الاستقلابية للسرطان:
السؤال الرئيسي:
هل الاستقلاب المرتفع للخلايا السرطانية نقطة ضعف يمكن استغلالها عن طريق التقييد الغذائي؟
تشمل الأسئلة الفرعية:
- ما هي المغذيات التي تغذي سرطانات محددة؟
- هل يجب تقييد تلك المغذيات؟
تدعم دراسات الفئران التدخلات الغذائية، لكن المتغيرات المربكة (مثل توقيت الوجبات) تعقد النتائج. ظهرت أنظمة محاكاة الصيام لمعالجة هذه المشكلة. ومع ذلك، لا يزال من غير الواضح أي نهج (مثل LFD، CR، FMD) أكثر فعالية. بينما وصلت LFD وCR إلى مراحل سريرية متقدمة، تنتظر FMD تجارب أكبر.
نظرًا للتوصيات القرآنية، نحث على إجراء تجارب معشاة ذات شواهد لاختبار فعالية الصيام الإسلامي إلى جانب التدخلات الاستقلابية الخاصة بكل موقع.
References:
- Longo, V.D., et al., Intermittent and periodic fasting, longevity and disease. Nature Aging, 2021. 1(1): p. 47-59.
- Prize, T.n., The Nobel Assembly at Karolinska Institutet has today decided to award the 2016 Nobel Prize in Physiology or Medicine to Yoshinori Ohsumi for his discoveries of mechanisms for autophagy. 2016, The nobel Prize.
- Kanarek, N., B. Petrova, and D.M. Sabatini, Dietary modifications for enhanced cancer therapy. Nature, 2020. 579(7800): p. 507-517.
- Caccialanza, R., et al., Fasting in oncology: a word of caution. Nature Reviews Cancer, 2019. 19(3): p. 177-177.
- Grimes, D.R. and E. O’Riordan, Starving cancer and other dangerous dietary misconceptions. The Lancet Oncology, 2023. 24(11): p. 1177-1178.
- Blaževitš, O., M. Di Tano, and V.D. Longo, Fasting and fasting mimicking diets in cancer prevention and therapy. Trends Cancer, 2023. 9(3): p. 212-222.
- de Groot, S., et al., Effects of short-term fasting on cancer treatment. J Exp Clin Cancer Res, 2019. 38(1): p. 209.
- de Groot, S., et al., Fasting mimicking diet as an adjunct to neoadjuvant chemotherapy for breast cancer in the multicentre randomized phase 2 DIRECT trial. Nat Commun, 2020. 11(1): p. 3083.
- Lu, Z., et al., Fasting selectively blocks development of acute lymphoblastic leukemia via leptin-receptor upregulation. Nature Medicine, 2017. 23(1): p. 79-90.
- Weng, M.-l., et al., Fasting inhibits aerobic glycolysis and proliferation in colorectal cancer via the Fdft1-mediated AKT/mTOR/HIF1α pathway suppression. Nature Communications, 2020. 11(1): p. 1869.
- Nencioni, A., et al., Fasting and cancer: molecular mechanisms and clinical application. Nat Rev Cancer, 2018. 18(11): p. 707-719.
- Vernieri, C., et al., Fasting-mimicking diet plus chemotherapy in breast cancer treatment. Nature Communications, 2020. 11(1): p. 4274.
- Zhang, J., Y. Deng, and B.L. Khoo, Fasting to enhance Cancer treatment in models: the next steps. Journal of Biomedical Science, 2020. 27(1): p. 58.
- Pomatto-Watson, L.C.D., et al., Daily caloric restriction limits tumor growth more effectively than caloric cycling regardless of dietary composition. Nature Communications, 2021. 12(1): p. 6201.
- Barradas, M., et al., Fatty acids homeostasis during fasting predicts protection from chemotherapy toxicity. Nature Communications, 2022. 13(1): p. 5677.
- Clifton, K.K., et al., Intermittent fasting in the prevention and treatment of cancer. CA Cancer J Clin, 2021. 71(6): p. 527-546.
- Khalifa, A., et al., Cyclic fasting bolsters cholesterol biosynthesis inhibitors’ anticancer activity. Nature Communications, 2023. 14(1): p. 6951.
- Marinac, C.R., et al., Prolonged Nightly Fasting and Breast Cancer Prognosis. JAMA Oncol, 2016. 2(8): p. 1049-55.
- Caffa, I., et al., Fasting-mimicking diet and hormone therapy induce breast cancer regression. Nature, 2020. 583(7817): p. 620-624.
- Sadeghian, M., et al., A review of fasting effects on the response of cancer to chemotherapy. Clin Nutr, 2021. 40(4): p. 1669-1681.
- Hanahan, D. and R.A. Weinberg, Hallmarks of cancer: the next generation. cell, 2011. 144(5): p. 646-674.
- Chandel, N.S., Glycolysis. Cold Spring Harbor Perspectives in Biology, 2021. 13(5): p. a040535.
- Chandel, N.S., Metabolism of proliferating cells. Cold Spring Harbor Perspectives in Biology, 2021. 13(10): p. a040618.
- Hui, S., et al., Glucose feeds the TCA cycle via circulating lactate. Nature, 2017. 551(7678): p. 115-118.
- Neinast, M.D., et al., Quantitative analysis of the whole-body metabolic fate of branched-chain amino acids. Cell metabolism, 2019. 29(2): p. 417-429. e4.
- DeBerardinis, R.J. and C.B. Thompson, Cellular metabolism and disease: what do metabolic outliers teach us? Cell, 2012. 148(6): p. 1132-1144.
- Reznik, E., et al., A landscape of metabolic variation across tumor types. Cell systems, 2018. 6(3): p. 301-313. e3.
- Ding, J., et al., A metabolome atlas of the aging mouse brain. Nature communications, 2021. 12(1): p. 6021.
- Ferraro, G.B., et al., Fatty acid synthesis is required for breast cancer brain metastasis. Nature cancer, 2021. 2(4): p. 414-428.
- Ngo, B., et al., Limited environmental serine and glycine confer brain metastasis sensitivity to PHGDH inhibition. Cancer discovery, 2020. 10(9): p. 1352-1373.
- Bi, J., et al., Altered cellular metabolism in gliomas—An emerging landscape of actionable co-dependency targets. Nature Reviews Cancer, 2020. 20(1): p. 57-70.
- Venneti, S. and C.B. Thompson, Metabolic reprogramming in brain tumors. Annual Review of Pathology: Mechanisms of Disease, 2017. 12(1): p. 515-545.
- Jung, Y., et al., The effect of sex hormones on normal breast tissue metabolism: Evaluation by FDG PET/CT. Medicine, 2019. 98(27): p. e16306.
- Monaco, M.E., Fatty acid metabolism in breast cancer subtypes. Oncotarget, 2017. 8(17): p. 29487.
- Marino, N., et al., Upregulation of lipid metabolism genes in the breast prior to cancer diagnosis. NPJ Breast Cancer, 2020. 6(1): p. 50.
- Sullivan, M.R., et al., Increased serine synthesis provides an advantage for tumors arising in tissues where serine levels are limiting. Cell metabolism, 2019. 29(6): p. 1410-1421. e4.
- André, F., et al., Alpelisib for PIK3CA-mutated, hormone receptor–positive advanced breast cancer. New England Journal of Medicine, 2019. 380(20): p. 1929-1940.
- Goncalves, M.D., B.D. Hopkins, and L.C. Cantley, Phosphatidylinositol 3-kinase, growth disorders, and cancer. New England Journal of Medicine, 2018. 379(21): p. 2052-2062.
- Saran, U., et al., Hepatocellular carcinoma and lifestyles. Journal of hepatology, 2016. 64(1): p. 203-214.
- Anstee, Q.M., et al., From NASH to HCC: current concepts and future challenges. Nature reviews Gastroenterology & hepatology, 2019. 16(7): p. 411-428.
- Jeon, J.Y., et al., Regulation of acetate utilization by monocarboxylate transporter 1 (MCT1) in hepatocellular carcinoma (HCC). Oncology Research, 2018. 26(1): p. 71.
- Lally, J.S., et al., Inhibition of acetyl-CoA carboxylase by phosphorylation or the inhibitor ND-654 suppresses lipogenesis and hepatocellular carcinoma. Cell metabolism, 2019. 29(1): p. 174-182. e5.
- Nakagawa, H., et al., Lipid metabolic reprogramming in hepatocellular carcinoma. Cancers, 2018. 10(11): p. 447.
- Healy, M.E., et al., Dietary sugar intake increases liver tumor incidence in female mice. Scientific Reports, 2016. 6(1): p. 22292.
- Tsuchida, T., et al., A simple diet-and chemical-induced murine NASH model with rapid progression of steatohepatitis, fibrosis and liver cancer. Journal of hepatology, 2018. 69(2): p. 385-395.
- Zhao, S., et al., Dietary fructose feeds hepatic lipogenesis via microbiota-derived acetate. Nature, 2020. 579(7800): p. 586-591.
- Taylor, S.R., et al., Dietary fructose improves intestinal cell survival and nutrient absorption. Nature, 2021. 597(7875): p. 263-267.
- Goncalves, M.D., et al., High-fructose corn syrup enhances intestinal tumor growth in mice. Science, 2019. 363(6433): p. 1345-1349.
- Yun, J., et al., Glucose deprivation contributes to the development of KRAS pathway mutations in tumor cells. Science, 2009. 325(5947): p. 1555-1559.
- Hao, Y., et al., Oncogenic PIK3CA mutations reprogram glutamine metabolism in colorectal cancer. Nature communications, 2016. 7(1): p. 11971.
- Brown, R.E., S.P. Short, and C.S. Williams, Colorectal cancer and metabolism. Current colorectal cancer reports, 2018. 14: p. 226-241.
- Satoh, K., et al., Global metabolic reprogramming of colorectal cancer occurs at adenoma stage and is induced by MYC. Proceedings of the National Academy of Sciences, 2017. 114(37): p. E7697-E7706.
- Pate, K.T., et al., Wnt signaling directs a metabolic program of glycolysis and angiogenesis in colon cancer. The EMBO journal, 2014. 33(13): p. 1454-1473.
- Oyama, N., et al., MicroPET assessment of androgenic control of glucose and acetate uptake in the rat prostate and a prostate cancer tumor model. Nuclear medicine and biology, 2002. 29(8): p. 783-790.
- Liu, Y., Fatty acid oxidation is a dominant bioenergetic pathway in prostate cancer. Prostate cancer and prostatic diseases, 2006. 9(3): p. 230-234.
- Cutruzzolà, F., et al., Glucose metabolism in the progression of prostate cancer. Frontiers in physiology, 2017. 8: p. 97.
- Davidson, S.M., et al., Environment impacts the metabolic dependencies of Ras-driven non-small cell lung cancer. Cell metabolism, 2016. 23(3): p. 517-528.
- Faubert, B. and R.J. DeBerardinis, Analyzing tumor metabolism in vivo. Annual Review of Cancer Biology, 2017. 1(1): p. 99-117.
- Davidson, S.M., et al., Direct evidence for cancer-cell-autonomous extracellular protein catabolism in pancreatic tumors. Nature medicine, 2017. 23(2): p. 235-241.
- Elia, I., et al., Breast cancer cells rely on environmental pyruvate to shape the metastatic niche. Nature, 2019. 568(7750): p. 117-121.
- Jang, C., et al., Metabolite exchange between mammalian organs quantified in pigs. Cell metabolism, 2019. 30(3): p. 594-606. e3.
- Zhang, A.M., et al., Endogenous hyperinsulinemia contributes to pancreatic cancer development. Cell metabolism, 2019. 30(3): p. 403-404.
- Lien, E.C., et al., Low glycaemic diets alter lipid metabolism to influence tumour growth. Nature, 2021. 599(7884): p. 302-307.
- Kamphorst, J.J., et al., Hypoxic and Ras-transformed cells support growth by scavenging unsaturated fatty acids from lysophospholipids. Proceedings of the National Academy of Sciences, 2013. 110(22): p. 8882-8887.
- Khasawneh, J., et al., Inflammation and mitochondrial fatty acid β-oxidation link obesity to early tumor promotion. Proceedings of the National Academy of Sciences, 2009. 106(9): p. 3354-3359.
- Frolova, A., et al., Facilitative glucose transporter type 1 is differentially regulated by progesterone and estrogen in murine and human endometrial stromal cells. Endocrinology, 2009. 150(3): p. 1512-1520.
- Cheung, L.W., et al., High frequency of PIK3R1 and PIK3R2 mutations in endometrial cancer elucidates a novel mechanism for regulation of PTEN protein stability. Cancer discovery, 2011. 1(2): p. 170-185.
- Memarzadeh, S., et al., Cell-autonomous activation of the PI3-kinase pathway initiates endometrial cancer from adult uterine epithelium. Proceedings of the National Academy of Sciences, 2010. 107(40): p. 17298-17303.
- Rutanen, E.-M., Insulin-like growth factors in endometrial function. Gynecological Endocrinology, 1998. 12(6): p. 399-406.
- Helmink, B.A., et al., The microbiome, cancer, and cancer therapy. Nature medicine, 2019. 25(3): p. 377-388.
- Weiss, E.P. and J.O. Holloszy, Improvements in Body Composition, Glucose Tolerance, and Insulin Action Induced by Increasing Energy Expenditure or Decreasing Energy Intake1. The Journal of nutrition, 2007. 137(4): p. 1087-1090.
- Heilbronn, L.K., et al., Effect of 6-month calorie restriction on biomarkers of longevity, metabolic adaptation, and oxidative stress in overweight individuals: a randomized controlled trial. Jama, 2006. 295(13): p. 1539-1548.
- Das, S.K., et al., Low or moderate dietary energy restriction for long‐term weight loss: What works best? Obesity, 2009. 17(11): p. 2019-2024.
- Rous, P., The influence of diet on transplanted and spontaneous mouse tumors. The Journal of experimental medicine, 1914. 20(5): p. 433-451.
- Castejón, M., et al., Energy restriction and colorectal cancer: a call for additional research. Nutrients, 2020. 12(1): p. 114.
- Pomatto-Watson, L.C., et al., Daily caloric restriction limits tumor growth more effectively than caloric cycling regardless of dietary composition. Nature communications, 2021. 12(1): p. 6201.
- Lv, M., et al., Roles of caloric restriction, ketogenic diet and intermittent fasting during initiation, progression and metastasis of cancer in animal models: a systematic review and meta-analysis. PloS one, 2014. 9(12): p. e115147.
- Orgel, E., et al., Caloric and nutrient restriction to augment chemotherapy efficacy for acute lymphoblastic leukemia: the IDEAL trial. Blood advances, 2021. 5(7): p. 1853-1861.
- de Man, F.M., et al., Effects of protein and calorie restriction on the metabolism and toxicity profile of irinotecan in cancer patients. Clinical Pharmacology & Therapeutics, 2021. 109(5): p. 1304-1313.
- Shaikh, H., et al., Body weight management in overweight and obese breast cancer survivors. Cochrane Database of Systematic Reviews, 2020(12).
- Goodwin, P.J., et al., Randomized trial of a telephone-based weight loss intervention in postmenopausal women with breast cancer receiving letrozole: the LISA trial. Journal of clinical oncology, 2014. 32(21): p. 2231-2239.
- Goodwin, P.J., et al., The LISA randomized trial of a weight loss intervention in postmenopausal breast cancer. NPJ Breast Cancer, 2020. 6(1): p. 6.
- Ligibel, J.A., et al., Randomized phase III trial evaluating the role of weight loss in adjuvant treatment of overweight and obese women with early breast cancer (Alliance A011401): study design. NPJ breast cancer, 2017. 3(1): p. 37.
- Pak, H.H., et al., Fasting drives the metabolic, molecular and geroprotective effects of a calorie-restricted diet in mice. Nature Metabolism, 2021. 3(10): p. 1327-1341.
- Mitchell, S.J., et al., Daily fasting improves health and survival in male mice independent of diet composition and calories. Cell metabolism, 2019. 29(1): p. 221-228. e3.
- Safdie, F.M., et al., Fasting and cancer treatment in humans: A case series report. Aging (Albany NY), 2009. 1(12): p. 988.
- Bauersfeld, S.P., et al., The effects of short-term fasting on quality of life and tolerance to chemotherapy in patients with breast and ovarian cancer: a randomized cross-over pilot study. BMC cancer, 2018. 18: p. 1-10.
- Jordan, S., et al., Dietary intake regulates the circulating inflammatory monocyte pool. Cell, 2019. 178(5): p. 1102-1114. e17.
- Trepanowski, J.F., et al., Effect of alternate-day fasting on weight loss, weight maintenance, and cardioprotection among metabolically healthy obese adults: a randomized clinical trial. JAMA internal medicine, 2017. 177(7): p. 930-938.
- Nencioni, A., et al., Fasting and cancer: molecular mechanisms and clinical application. Nature Reviews Cancer, 2018. 18(11): p. 707-719.
- Wei, M., et al., Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and cardiovascular disease. Science translational medicine, 2017. 9(377): p. eaai8700.
- Sadeghian, M., et al., Effect of fasting-mimicking diet or continuous energy restriction on weight loss, body composition, and appetite-regulating hormones among metabolically healthy women with obesity: a randomized controlled, parallel trial. Obesity Surgery, 2021. 31: p. 2030-2039.
- Salvadori, G., et al., Fasting-mimicking diet blocks triple-negative breast cancer and cancer stem cell escape. Cell metabolism, 2021. 33(11): p. 2247-2259. e6.
- Di Tano, M., et al., Synergistic effect of fasting-mimicking diet and vitamin C against KRAS mutated cancers. Nature Communications, 2020. 11(1): p. 2332.
- Valdemarin, F., et al., Safety and feasibility of fasting-mimicking diet and effects on nutritional status and circulating metabolic and inflammatory factors in cancer patients undergoing active treatment. Cancers, 2021. 13(16): p. 4013.
- Bianchi, G., et al., Fasting induces anti-Warburg effect that increases respiration but reduces ATP-synthesis to promote apoptosis in colon cancer models. Oncotarget, 2015. 6(14): p. 11806.
- Liu, Y.P., et al., Molecular mechanisms of chemo‐and radiotherapy resistance and the potential implications for cancer treatment. MedComm, 2021. 2(3): p. 315-340.
- Wang, Y., et al., Involvement of CUL4A in regulation of multidrug resistance to P-gp substrate drugs in breast cancer cells. Molecules, 2013. 19(1): p. 159-176.
- Vingeliene, S., et al., An update of the WCRF/AICR systematic literature review and meta-analysis on dietary and anthropometric factors and esophageal cancer risk. Annals of Oncology, 2017. 28(10): p. 2409-24.
- Valiahdi, S.M., M. Iranshahi, and A. Sahebkar, Cytotoxic activities of phytochemicals from Ferula species. DARU Journal of Pharmaceutical Sciences, 2013. 21: p. 1-7.
- Tey, J., et al., Palliative radiotherapy for gastric cancer: a systematic review and meta-analysis. Oncotarget, 2017. 8(15): p. 25797.
- Sung, H., et al., Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 2021. 71(3): p. 209-249.
- Smalley, S.R., et al., Updated analysis of SWOG-directed intergroup study 0116: a phase III trial of adjuvant radiochemotherapy versus observation after curative gastric cancer resection. Journal of clinical oncology, 2012. 30(19): p. 2327-2333.
- Roshandel, G., et al., Cancer in Iran 2008 to 2025: recent incidence trends and short‐term predictions of the future burden. International journal of cancer, 2021. 149(3): p. 594-605.
- Rocco, A., et al., MDR1-P-glycoprotein behaves as an oncofetal protein that promotes cell survival in gastric cancer cells. Laboratory investigation, 2012. 92(10): p. 1407-1418.
- Mao, Z., et al., Tamoxifen reduces P-gp-mediated multidrug resistance via inhibiting the PI3K/Akt signaling pathway in ER-negative human gastric cancer cells. Biomedicine & Pharmacotherapy, 2014. 68(2): p. 179-183.
- Lippert, T.H., H.-J. Ruoff, and M. Volm, Intrinsic and acquired drug resistance in malignant tumors. Arzneimittelforschung, 2008. 58(06): p. 261-264.
- Kozovska, Z., V. Gabrisova, and L. Kucerova, Colon cancer: cancer stem cells markers, drug resistance and treatment. Biomedicine & Pharmacotherapy, 2014. 68(8): p. 911-916.
- Katayama, K., et al., Inhibition of the mitogen-activated protein kinase pathway results in the down-regulation of P-glycoprotein. Molecular cancer therapeutics, 2007. 6(7): p. 2092-2102.
- Zhang, J., et al., ATM functions at the peroxisome to induce pexophagy in response to ROS. Nature cell biology, 2015. 17(10): p. 1259-1269.
- Szumiel, I., Ionizing radiation-induced oxidative stress, epigenetic changes and genomic instability: the pivotal role of mitochondria. International journal of radiation biology, 2015. 91(1): p. 1-12.
- Iranshahi, M., et al., Sesquiterpene coumarins from Ferula szowitsiana and in vitro antileishmanial activity of 7-prenyloxycoumarins against promastigotes. Phytochemistry, 2007. 68(4): p. 554-561.
- Iangcharoen, P., et al., Anti-P-glycoprotein conjugated nanoparticles for targeting drug delivery in cancer treatment. Archives of pharmacal research, 2011. 34: p. 1679-1689.
- Helleday, T., et al., DNA repair pathways as targets for cancer therapy. Nature Reviews Cancer, 2008. 8(3): p. 193-204.
- Gottesman, M.M., T. Fojo, and S.E. Bates, Multidrug resistance in cancer: role of ATP–dependent transporters. Nature reviews cancer, 2002. 2(1): p. 48-58.
- de Oliveira, J., et al., Association between ABCB1 immunohistochemical expression and overall survival in gastric cancer patients. Asian Pacific journal of cancer prevention, 2014. 15(16): p. 6935-6938.
- Cunningham, D., et al., Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. New England Journal of Medicine, 2006. 355(1): p. 11-20.
- Catalano, V., et al., Gastric cancer. Critical reviews in oncology/hematology, 2009. 71(2): p. 127-164.
- Mesci, A. and R.K. Wong, Current and future strategies for radiation therapy in gastric cancer. Journal of Surgical Oncology, 2022. 125(7): p. 1161-1175.
- Vernieri, C., et al., Fasting-mimicking diet is safe and reshapes metabolism and antitumor immunity in patients with cancer. Cancer Discovery, 2022. 12(1): p. 90-107.
- Dorff, T.B., et al., Safety and feasibility of fasting in combination with platinum-based chemotherapy. BMC cancer, 2016. 16: p. 1-9.
- de Groot, S., et al., The effects of short-term fasting on tolerance to (neo) adjuvant chemotherapy in HER2-negative breast cancer patients: a randomized pilot study. BMC cancer, 2015. 15: p. 1-9.
- Vernieri, C., et al., Exploiting fasting-mimicking diet and metformin to improve the efficacy of platinum-pemetrexed chemotherapy in advanced LKB1-inactivated lung adenocarcinoma: the FAME trial. Clinical lung cancer, 2019. 20(3): p. e413-e417.
- Cohen, C.W., et al., A ketogenic diet reduces central obesity and serum insulin in women with ovarian or endometrial cancer. The Journal of nutrition, 2018. 148(8): p. 1253-1260.
- Cohen, C.W., et al., Favorable effects of a ketogenic diet on physical function, perceived energy, and food cravings in women with ovarian or endometrial cancer: a randomized, controlled trial. Nutrients, 2018. 10(9): p. 1187.
- Cohen, C.W., et al., A ketogenic diet is acceptable in women with ovarian and endometrial cancer and has no adverse effects on blood lipids: a randomized, controlled trial. Nutrition and cancer, 2020. 72(4): p. 584-594.
- McGuire, S., US department of agriculture and US department of health and human services, dietary guidelines for Americans, 2010. Washington, DC: US government printing office, January 2011. Advances in nutrition, 2011. 2(3): p. 293-294.
- Evert, A.B., et al., Nutrition therapy recommendations for the management of adults with diabetes. Diabetes care, 2014. 37(Supplement_1): p. S120-S143.
- Lichtenstein, A.H., et al., 2021 dietary guidance to improve cardiovascular health: a scientific statement from the American Heart Association. Circulation, 2021. 144(23): p. e472-e487.
- Sacks, F.M., et al., Soy protein, isoflavones, and cardiovascular health: an American Heart Association Science Advisory for professionals from the Nutrition Committee. Circulation, 2006. 113(7): p. 1034-1044.
- Chlebowski, R.T., et al., Low-fat dietary pattern and breast cancer mortality in the Women’s Health Initiative randomized controlled trial. Journal of Clinical Oncology, 2017. 35(25): p. 2919-2926.
- Chlebowski, R.T., et al., Association of low-fat dietary pattern with breast cancer overall survival: a secondary analysis of the women’s health initiative randomized clinical trial. JAMA oncology, 2018. 4(10): p. e181212-e181212.
- Thomson, C.A., et al., Cancer incidence and mortality during the intervention and postintervention periods of the Women’s Health Initiative dietary modification trial. Cancer Epidemiology, Biomarkers & Prevention, 2014. 23(12): p. 2924-2935.
- Chlebowski, R.T., et al., Dietary fat reduction and breast cancer outcome: interim efficacy results from the Women’s Intervention Nutrition Study. Journal of the National Cancer Institute, 2006. 98(24): p. 1767-1776.
- Pierce, J.P., et al., Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: the Women’s Healthy Eating and Living (WHEL) randomized trial. Jama, 2007. 298(3): p. 289-298.
- Rock, C.L., et al., Effects of a high-fiber, low-fat diet intervention on serum concentrations of reproductive steroid hormones in women with a history of breast cancer. Journal of Clinical Oncology, 2004. 22(12): p. 2379-2387.
- Labbé, D.P., et al., High-fat diet fuels prostate cancer progression by rewiring the metabolome and amplifying the MYC program. Nature communications, 2019. 10(1): p. 4358.
- Gao, X., et al., Dietary methionine influences therapy in mouse cancer models and alters human metabolism. Nature, 2019. 572(7769): p. 397-401.
- Safdie, F., et al., Fasting enhances the response of glioma to chemo-and radiotherapy. 2012.
- Allen, B.G., et al., Ketogenic diets enhance oxidative stress and radio-chemo-therapy responses in lung cancer xenografts. Clinical Cancer Research, 2013. 19(14): p. 3905-3913.
- Voss, M., et al., ERGO2: a prospective, randomized trial of calorie-restricted ketogenic diet and fasting in addition to reirradiation for malignant glioma. International Journal of Radiation Oncology* Biology* Physics, 2020. 108(4): p. 987-995.